
Most Popular
-
1
[AtoZ into Korean mind] Humor in Korea: Navigating the line between what's funny and not
![[AtoZ into Korean mind] Humor in Korea: Navigating the line between what's funny and not](//res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/22/20240422050642_0.jpg&u=)
-
2
[Exclusive] Korean military set to ban iPhones over 'security' concerns
![[Exclusive] Korean military set to ban iPhones over 'security' concerns](//res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/23/20240423050599_0.jpg&u=20240423183955)
-
3
Yoon seeks rebound, taps 5-term lawmaker as chief of staff

-
4
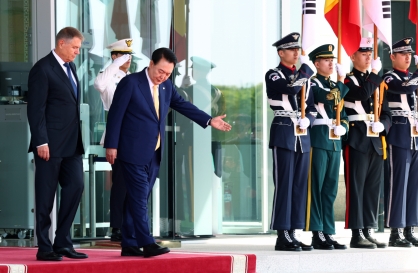
Korean, Romanian leaders discuss defense tech, nuclear energy
-
5
Medical standoff deepens as doctors reject new med school plan, talks

![[AtoZ into Korean mind] Humor in Korea: Navigating the line between what's funny and not](http://res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/22/20240422050642_0.jpg&u=)
![[Exclusive] Korean military set to ban iPhones over 'security' concerns](http://res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/23/20240423050599_0.jpg&u=20240423183955)



-
6
[Graphic News] 77% of young Koreans still financially dependent
![[Graphic News] 77% of young Koreans still financially dependent](//res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/22/20240422050762_0.gif&u=)
-
7
[Herald Interview] Why Toss invited hackers to penetrate its system
![[Herald Interview] Why Toss invited hackers to penetrate its system](//res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/22/20240422050569_0.jpg&u=20240422150649)
-
8
S. Korean envoys convene to navigate strategy amid Middle East tensions

-
9
S. Korea calls on Japan to confront history amid Yasukuni Shrine visit

-
10
North Korea fires several short-range ballistic missiles into sea: JCS

![[Graphic News] 77% of young Koreans still financially dependent](http://res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/22/20240422050762_0.gif&u=)
![[Herald Interview] Why Toss invited hackers to penetrate its system](http://res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/22/20240422050569_0.jpg&u=20240422150649)



WASHINGTON (AP) ― The government’s top drug abuse experts struggled Wednesday to find ways to expand use of a medicine which is widely-considered the best therapy for treating heroin and painkiller addiction, but which remains underused a decade after its launch.
Sen. Carl Levin of Michigan pressed officials from the White House, the National Institute of Drug Abuse and other agencies to increase access to the buprenorphine, a medication which helps addicts control drug cravings and withdrawal symptoms.
First approved in 2002 ― under a law crafted by Levin and Utah Republican Sen. Orrin Hatch ― buprenorphine was hailed as a major advance over methadone, the decades-old standard for addiction treatment.
Sen. Carl Levin of Michigan pressed officials from the White House, the National Institute of Drug Abuse and other agencies to increase access to the buprenorphine, a medication which helps addicts control drug cravings and withdrawal symptoms.
First approved in 2002 ― under a law crafted by Levin and Utah Republican Sen. Orrin Hatch ― buprenorphine was hailed as a major advance over methadone, the decades-old standard for addiction treatment.

Among other advantages, buprenorphine has lower risk of overdose, milder side effects and can be prescribed as a take-home medication in the privacy of a doctor’s office ― avoiding the stigma of going to a methadone clinic.
But even amid the national epidemic of drug abuse and addiction, access to the buprenorphine remains limited by federal restrictions, inconsistent insurance coverage and a lack of acceptance by physicians.
“As long as we have too few doctors certified to prescribe bupe, we will be missing a major weapon in the fight against the ravages of addiction,” Levin told the forum, which also included patients and non-government medical experts.
Only 4 percent of the 625,000 U.S. doctors who are eligible to prescribe buprenorphine have received certification to use the drug ― which comes as a pill or a film that dissolves under the tongue. Certification requires an eight hour training course in addiction medicine.
Meanwhile an estimated 2.5 million Americans are addicted to prescription painkillers or heroin, known collectively as opioids, and less-than half are receiving medical treatment.
“It‘s somewhat paradoxical that physicians will use opioids to create a problem, but there seems to be reluctance to help address the problem,” said Dr. Westley Clark of the Center for Substance Abuse Treatment. Clark and other experts noted that there is still a stigma attached to treating opioid addiction and many physicians are uninterested in learning how to use drugs like buprenorphine.
Government officials agreed that more training is needed to familiarize both medical students and established physicians with the science that shows addiction can be successfully treated with medication.
Even among doctors who are certified to prescribe buprenorphine, federal law caps the number of patients they can treat to 100.
Dr. Corey Waller, an addiction specialist from Grand Rapids, Michigan, said he has a constant waiting list of patients trying to get a prescription.
“It’s the only medication that has a limit of treatment capability out of all the medicines in the U.S.,” said Waller, who also spoke on behalf of the American Society of Addiction Medicine. The group has proposed raising the patient cap to as high as 500 patients for physicians who complete 40 hours of training.
But federal officials cautioned against that approach, noting that buprenorphine itself can be abused.
Dr. Nora Volkow, director of the National Institute on Drug Abuse, noted that buprenorphine overdoses are routinely reported in Europe, where the drug is less restricted. Other officials warned that raising the prescribing limit might lead to buprenorphine pill mills, where rogue doctors prescribe drugs in exchange for money from addicts.
Methadone and buprenorphine are themselves opioids, part of that class of highly-addictive drugs that mimic the effect of the opium poppy. When dosed carefully though, both drugs can reduce opioid withdrawal symptoms ― including anxiety, sweating, nausea and vomiting ― without the euphoric high seen with drugs like heroin.
Despite similarities between methadone and buprenorphine, doctors and recovering addicts agree buprenorphine has clear benefits. Patients report less fatigue and mental fogginess on the newer drug. Most significantly, buprenorphine can be prescribed in an extended take-home supply, freeing patients from making daily trips to methadone clinics.
“It’s a drug that allows us to lead a normal life,” said Dr. John Kitzmiller, a Michigan doctor who recovered from this own opioid addiction using buprenorphine. “You can’t live a normal life on methadone.”

![[Exclusive] Korean military to ban iPhones over security issues](http://res.heraldm.com/phpwas/restmb_idxmake.php?idx=652&simg=/content/image/2024/04/23/20240423050599_0.jpg&u=20240423183955)



![[Today’s K-pop] Ateez confirms US tour details](http://res.heraldm.com/phpwas/restmb_idxmake.php?idx=642&simg=/content/image/2024/04/23/20240423050700_0.jpg&u=)